

The “put me back, I don’t like it out here” cry of a newborn. I choose this icon as representative of the AMA’s reaction to the merest possibility that it might have to give up it’s historically-based exploitive behavior as described in this essay and its many links to supporting materials.
Easy-to-share Tiny URL: https://tinyurl.com/y3g3v8vk
Mandatory Physician Supervision &
Mandatory Physician Referral:
Two sides of the very same coin
The name of that ‘coin’ is “borrowed servant/captain-of-the-ship”. For over a century the US legal system has described the relationship between medical doctors and non-MD assistants as one in which the doctor is identified as the “Captain of the ship”, while nurses and other types of non-MD ‘helpers’ and ‘assistants’ are considered to be the doctor’s “borrowed servants“.
A more modern version of this idea is provided to us by the AMA in its “Scope of Practice PArtnership” (SOPP) in its House of Delegates Resolution H-35-973″
H-35.973 Scopes of Practice of Physician Extenders
Our AMA supports the formulation of clearer definitions of the scope of practice of physician extenders to include direct appropriate physician supervision and recommended guidelines for physician supervision to ensure quality patient care. (Res. 213, A-02)
 NOTE: Longer excerpt of the AMA’s SOPP are provided at the end of this essay, followed by a number of links to historically pertinent documents.
NOTE: Longer excerpt of the AMA’s SOPP are provided at the end of this essay, followed by a number of links to historically pertinent documents.
Here is a link from another website that posts the full text of the AMA’s response to Ricki Lake and her film “The Business of Being Born”

A nurse focusing the light for the doctor
Definition of “Borrowed Servant/Captain-of-the-Ship“
Legal scholars typically refer to this as a legal theory that holds doctors with hospital practice privileges (i.e. independent contractors) financially responsible for the actions of subservient hospital employees acting under the doctor’s authority and/or direction.
For example, it would apply to nurses, aids, orderlies who are carrying out the “Doctor’s Orders”when they provide bedside patient care and circulating and scrub nurses who assisted doctors during surgical procedures, normal birth, forceps deliveries and C-sections.
In event of a malpractice suit, the “Captain of the Ship”physician (but not the hospital) would be held responsible for monetary damages, even when the harm was the result of errors made by nurses or other assistants who were under control of the doctor/captain.
Now days, hospitals have their own medical malpractice coverage, so this legal principle is rarely used.
However, “Borrowed Servant-Captain of the Ship” also perfectly reflects the elevated social status and power dynamics of the allopathic medical profession. Seeing all non-physicians as doctor-helpers goes back more than a century ago, to a group of individual who considered themselves to be an aristocracy of white, upper-class, college-educated men who naturally enjoyed the privileges associated with their elevated social status.
This hierarchical model sees nurses, nurse-midwives and, after passage of AB 1308 in 2013, licensed midwives as a subservient class of “underlings” — borrowed servants whose role and “raison d’etre” is to support the medical profession, no matter how poorly they pay us, or how badly they treat us.
The hierarchical plan of organized medicine is plainly laid out in California’s 1974 CNM licensing law and in the original 1993 LMPA (which also mandated physician supervision provision) and now in the mandatory physician referral in AB 1308.
Obviously there are important differences btw mandated physician supervision and mandated physician referral. The ladder affects midwives less frequently and impacts a smaller number of mothers; nonetheless, the only difference between the two is in the number of people affected.
When it comes to exercising unilateral control over midwives and childbearing women, mandated referral is the same expression of unearned control over others as was mandatory supervision of Ca LM and continues to be the case for Ca CNMs.
 AB 1308 drastically reduced the professional role of Ca LMs by shifting their professional decision-making role to the obstetrical profession
AB 1308 drastically reduced the professional role of Ca LMs by shifting their professional decision-making role to the obstetrical profession

AB 1308 displaced the traditional process of professional collaboration, which began with consultation — between midwives and with other maternity care professionals.
It did this by repealing the Standard of Care of California Licensed Midwives (SCLLM), which defined the role of LMs relative to the clients who wanted obstetrical evaluations or needed to transfer care.
AB 1308 legally replaced its detailed and informative language of the SCCLM with a “one-size-fits-all” mandatory physician referral for “any deviation from norm” (even when not clinically significant & without the mother’s consent), as well as a single list of 26 “Thou Shalt Nots” that was specifically chosen to replace the very informative 14-page SCLLM.
When you read the language of the SCLLM, it’s easy to see its value and what we and childbearing families lost by its repeal. THe SCCLM was authorized by SB 1950 in 2002, adopted by the MBC in 2005, approved by the OAL in March of 2006 and functioned without a glitch during the 8 years that preceded its abrupt repeal by AB 1308.
Here are just a few of the most pertinent excerpts of the SCLLM, beginning with:
Section II: “Brief overview of the licensed midwife’s duties and specific responsibilities to childbearing women and their unborn and newborn babies“
A. The California licensed midwife engages in an ongoing process of risk assessment that begins with the initial consultation and continues throughout the provision of care.
This includes continuously assessing for normalcy and, if necessary, initiating appropriate interventions including consultation, referral, transfer, first-responder emergency care and/or emergency transport.
STANDARD SIX ~ The Midwife shall confer and collaborate with other healthcare professionals, including other midwives, as is necessary to professionally meet the client’s needs.
When the client’s condition or needs exceed the Midwife’s scope of practice or personal practice guidelines, the Midwife shall consult with and refer to a physician or other appropriate healthcare provider.
V. Risk factors identified during the initial interview or arising during the course of care
A. Responsibility of the Licensed Midwife
With respect to the care of a client with a significant risk factor as identified by the client selection criteria in section IV or other science-based parameters, the licensed midwife shall inform the client about the known material risks and benefits of continuing with midwifery care relative to the identified risk factor and shall recommend to the client that her situation be evaluated by a medical practitioner and if appropriate, to transfer her primary care to a licensed physician who has current training and practice in obstetrics.
H Client’s Rights to Self-Determination
In recognition of the client’s right to refuse that recommendation as well as other risk-reduction measures and medical procedures, the client may, after having been fully informed about the nature of the risk and specific risk-reduction measures available, make a written informed refusal.
If the licensed midwife appropriately documents the informed refusal in the client’s midwifery records, the licensed midwife may continue to provide midwifery care to the client consistent with evidence-based care as identified in this document and the scientific literature.

Capital Building, Sacramento, Ca
How AB 1308 subverted the professional role of Ca LMs
AB 1308 subverted and in certain cases, eliminated the professional role of licensed midwives by declaring that any childbearing woman with a risk-factor or a possible ‘deviation from normal’ is no longer eligible to be the midwife’s client until after she has first become the patient of an obstetrician.
At that point, it’s up to the obstetrical provider to decide whether or not the CB woman will be “allowed” to resume her midwifery care. This decision can be based on anything or nothing, since the law provides no factual guidance and no penalty for malfeasance if the OB should rule her ineligible for midwifery care ‘without merit’ or simply to protect themself from a “vicarious” liability lawsuit.
Notice how all “roads lead (back) to Rome” in that all control and decision-making comes back to MDs as being at the top of the food chain.

A Brief Trip in the “Way-Back Machine”
“To Cure Without Studying” ~ Historic definition of the illegal practice of medicine:
Historically, the medical profession has promoted two ideas that have nothing to do with the healing of the sick, or other compassionate functioning a medical doctors.
The first was their insistence that only men had the intellect, unsentimental temperament, and stamina to be doctors.
{Note-2-self ~ add link to 1822 source document by a physician entitled “On Female Practitioners of Midwifery”}
The second was that “medical men” (which is whnt doctors preferred to be called) and only medical men (i.e. allopathically-trained MDs) should have absolute and permanent control over the entity of the practice of medicine.
This was negatively defined by claiming that it was an illegal practice of medicine“to cure without having studied” .
Doctors weren’t arguing that care provided by non-MD practitioner failed to cure the patient or that their care somehow harmed their patients, just that it was illegal for any non-MD to provide any type of health-related care without first graduating from one of the allopathic medical schools approved by the AMA’s Flexner Report on published by the Rockefeller Foundations in 1910. Not only did you have to be a MD but you could not provide any form of care that did not fall into the definition of allopathic medicine — i.e. the use of Rx drugs, surgery and ionizing radiation.
So midwives, naturopaths, herbolists, and many other healthcare disciplines were summarily eliminated from what we now refer to as “healthcare” but in fact is an allopathic medical services delivery system (i.e. MSDS). Our MSDS is great if you are in an accident or develop an acute disease, but what has been ‘systemized’ is not ‘caring’ for our ‘health’.
I’m not suggesting that healthcare providers don’t need to be safe, which is to say knowledgable practitioners — educated, clinically-trained, state-regulated. I’m pointing out that the current hierarchical system is a 19th century dinosaur based on a 19th century gender prejudice that basically said “you girls can’t play with our “boy toys” unless we give you a very special (and limited) dispensation as a nurse acting under the supervision of an MD”.
American obstetrics, which is a surgical specialty, historically defined pregnancy as a 9-month disease that required a surgical cure. When an early 20th century midwife provided care during the biological process of labor and birth, organized medicine saw this “curing” of pregnant women, which was an illegal practice of medicine.
Next Stop on the Way-Back Machine:
Problem: How can the average doctor make his obstetrical medicine practice profitable?
Solution:
First, redefined normal vaginal ‘birth’ as a surgical procedure that can only be “performed” by male physician-surgeons on a labor patient rendered unconscious by general anesthesia and “conducted” with the same level of sterile protocols as used for major abdominal surgery.
Then have the hospital’s low-paid, all-female nursing staff provide all the care during the many hours of labor, as well as the immediate and routine postpartum, while holding L&D nurses responsible for calling the doctor at the right time to ‘deliver’ the baby. {Note: I was an L&D over the course of 15 years and know of what i speak!}
This empowers doctors to get really mad at the nurse (even get her fired) if she didn’t call at precisely the right moment — not too soon (i.e. wasting his time!), and not too late. This is the most critical, as not being in the room when the baby is born legally prevents billing for having “conducted the delivery” under the surgical billing code ‘NSVD’ (normal spontaneous vaginal delivery).
Below are several historical quoted by obstetricians published in 1911 & 1922. They plainly identify the reason and role of the doctor’s subservient assistants and explain the politics of organized medicine (like ACOG) that are still rule the day.
“The doctor must be enabled to get his money from small fees received from a much larger number of patients cared for under time-saving and strength-conserving conditions;
… he must do his work at the minimum expense to himself, and he must not be asked to do any work for which he is not paid the stipulated fee.
This means … doctors must be relieved of all work that can be done by others — nurses, social workers, and midwives.” [1922-A; ZieglerMD, p. 412]
“The nurses should be trained to do all the antepartum and postpartum work, from both the doctors’ and nurses’ standpoint, with the doctors always available as consultants when things go wrong; and the midwives should be trained to do the work of the so called “practical nurses,” acting as assistants to the regular nurses and under their immediate direction and supervision, and to act as assistant-attendants upon women in labor—conducting the labor during the waiting period or until the doctor arrives, and assisting him during the delivery.” [1922-A; ZieglerMD]
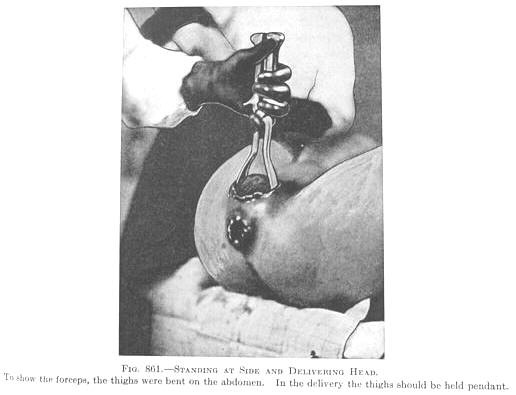
In order to follow the natural 60-degree curve of the childbearing pelvis, the obstetrician must to pull straight up towards the ceiling with the forceps in order to deliver the baby’s head
“In this plan the work of the doctors would be limited to the delivery of patients, consulting with the nurses, and to the making of complete physical and obstetrical examinations … [1922-A; ZieglerMD, p. 413]
“What we must first do is arouse public sentiment and first of all we must have the enthusiastic support and united action of the medical fraternity.…
We feel that the most important change should be in the laws governing the registration of births. The word “midwife” as it occurs, should be at once erased from the statute books. …
We believe it to be the duty and privilege of the medical profession of American to safeguard the health of the people; we believe it to be the duty and privilege of the obstetricians of our country to safeguard the mother and child in the dangers of childbirth.
Dr. J. Whitridge Williams, author of “Williams Obstetrics” first published in 1904. After graduating from medical school in 1886, he trained as a gynecological surgeon, then spent 2 yrs in Europe in obstetrical and pathology clinical training programs. He was appointed Chief of Obstetrics at Johns Hopkins in 1899, and Dean of the Johns Hopkin’s School of Medicine in 1911. His book “Twilight Sleep: Simple Discoveries in Painless Childbirth” was published in 1914. His big dream was to find a reliable way to finance a national system of general hospitals like the ones available for 200 years in Western Europe. However, the AMA would never tolerate anything like the national systems paid for and often run by a national government. In an effort to generate a new and reliable revenue stream that could be used over the next decades to expand small privately-owned hospitals and build and equip new community general hospitals – one for every population center over 3,000 — and described by Dr. W “to as ubiquitous if not quite of numerous as libraries and school houses”). To pay for this he came up with the idea of ‘elective hospitalization’. He saw this as creating a large and steady stream of paying customers. The first demographic for elective hospitalizations were healthy middle- and upper-class maternity patients whose families well could afford to pay both the doctors’ fee a AND a hospital bill for a 14-day stay of mother in the maternity ward and the baby in the newborn nursery. Just one hospital labor and birth a day, with a 14-day stay for both mother and baby (total of 28 hospital days per birth) & equated to a maternity department pt. census of 9,800 days per year. Inventing this income stream was an extraordinarily clever way generate money that would circumvent the politics of the AMA. Organized medicine in the US was opposed to anything that might interfere with its entrepreneurial view of medicine as a very lucrative & ‘no-holds-barred’ small business that could generate consider wealth from private physician fees. The AMA also rejected anything that smacked of “gov’t” meddling in the practice of medicine, which rejection of state or federal gov’t financing. The AMA equated this to gov’t -run ‘socialized medicine’, which it hated. Without access to the non-gov’t sources of revenue from hospitalized healthy maternity patients, Dr. J. W. Williams knew the AMA would have killed his life-long dream — a nationwide system of well equipped , well-staffed general hospitals. From that standpoint, Dr. Williams scheme was masterful and he succeeded beyond his wildest dreams. What this meant for healthy childbearing women is a story for another day (see list of Tiny URLs at the bottom of this post that lead to the Dr. JWW’s personal and professional story)
The obstetricians are the final authority to set the standard and lead the way to safety. They alone can properly educate the medical profession, the legislators and the public.” {*Boston Medical and Surgical Journal, Feb. 23, 1911, page 261}
In this system, MDs make all the decisions about what is to be done — drugs to be administered (how much and when), whether the patient is ‘allowed’ out of bed, what he or she can eat or do. Doctors convey this to the nursing staff via “Doctors Orders” and various “standing orders” and hospital protocols developed by the MD department chief. These policies and protocols outline what nurses are allowed to do without having to first call the doctor to get a specific “order”.

The nurse holds the patient’s legs, while the doctor does the vaginal exam
The original supervision provision in California’s nurse-mfry law mirrored this same hierarchical system that has began defining the status and power arrangement between male doctors and female nurses since Florence Nightingale invented the modern role of professional nursing during the Crimean War best described as “physician-helpers” or a non-sexual version of a dedicated and dutiful wife who made it possible for battle surgeons to save lives.
‘Essential Workers’, circa 2020
Like mothers, cooks, bus drivers, janitors, and nannies, nurses became what we today (covid-19 era) call ‘essential workers’ — disproportionally-female service workers who are vitally necessary to keep the “system” running — delivery of goods and services, the bedpans hospital patients emptied, babies diapered, buses on time, school cafeterias serving nutritious meals, etc. While the work is literally life-saving, these essential workers are poorly paid, unappreciated, and labor under stressful conditions over which that they have little or no control.
 Before returning to the contemporary topic of AB 1308, I must note that our medical services delivery system — most especially the care of hospitalized patients — would come to an instant standstill if the system was required to be fair and equatable — that is if:
Before returning to the contemporary topic of AB 1308, I must note that our medical services delivery system — most especially the care of hospitalized patients — would come to an instant standstill if the system was required to be fair and equatable — that is if:
- (a) doctors had to personally provide all the care each of their private patients required over each 24 hour period
OR - (b) had to pay wages of equivalent value to nurses and other employees that make the hospital system work 24 hrs a day, 365 days a year. It should be noted that access to all these services are totally free to MDs with hospital practice privileges. Think of all the services a major airport provides to the people who pass through it and yet pay nothing for all its amenities.
Jumping 150 years ahead to present time, modern-day nurse-midwives are legally permitted to be “independent contractors” instead of just employees for a doctor or hospital, but idea of ‘independence’ for nurse-midwives stops there.
In order to keep these ICs (independent contractors) in their ‘appropriately ‘ subservient place in the medical hierarchy, CNMs are only allowed to provide midwifery care while working under the thumb a supervising obstetrician. If the owners of those “thumbs” refuse to supervise, CNMs in California cannot attend births or otherwise legally practice midwifery.
The CMA achieved this great feat by mandating a written “practice agreement” in which each supervising obstetrician defines what the nurse-midwife he or she supervised could and couldn’t do, who she could provide care to and also outline the circumstances in which the CNM must “call the doctor” to get permission to provide (or continue providing) care. This included being ordered by her supervising obstetrician to refer or transfer care or have her client admitted to the hospital OB department, even if the mother did not voluntarily consent to this course of action (ex. 42 wks w/ normal AFI and reassuring fetal heart rate).
AB 1308 achieved many of the same goals as the 1974 CNM law by negating the inherent independence in the LMPA as written by Senator Lucy Killea in 1993 and putting the profession of licensed midwifery under the medical profession’s hierarchal system in the same subservient status as nurses and California nurse-midwives.
 The professional independence in the original SB 350 (LMPA) was conveyed in statutory language that defined our scope of practice as “attending cases of normal childbirth“ (as well as authorizing antepartum, postpartum, neonatal, and ‘inter-conceptional’ care & family planning).
The professional independence in the original SB 350 (LMPA) was conveyed in statutory language that defined our scope of practice as “attending cases of normal childbirth“ (as well as authorizing antepartum, postpartum, neonatal, and ‘inter-conceptional’ care & family planning).
SB 350 also limited the practice of licensed midwifery to essentially healthy CB women who were not suffering from any clinically significant (i.e. present-tense) complication, in which case immediate transfer by the midwife to physician care was required.
After having used the descriptive phase “cases of normal childbirth” to define our scope of practice, SB 350 identified ‘abnormal‘ childbirth the limit of that scope of practice. This was defined as any situation that called for the use of “artificial, mechanical and forcible means”. Employment of them is considered to be a practice of medicine. The LMPA plainly states that the “license to practice midwifery does not permit the holder to practice medicine or surgery“.
 AB 1308 took control away from mothers by totally ignoring patient autonomy and rights of informed consent and informed refusal. It drastically diminished the professional status of licensed midwifery by cannibalizing the LMPA’s scope of practice, eliminating the Standard of Care for California Licensed Midwives (SCCLM — SB 1950) and substituting a totally negative list of 24 ‘no-no’s (what LMs can’t do). A list of what midwies CAN’T DO is neither a standard of care, or a useful practice guideline.
AB 1308 took control away from mothers by totally ignoring patient autonomy and rights of informed consent and informed refusal. It drastically diminished the professional status of licensed midwifery by cannibalizing the LMPA’s scope of practice, eliminating the Standard of Care for California Licensed Midwives (SCCLM — SB 1950) and substituting a totally negative list of 24 ‘no-no’s (what LMs can’t do). A list of what midwies CAN’T DO is neither a standard of care, or a useful practice guideline.
This statutory scheme of ANB 1308 eliminated the midwife’s professional decision-making process that traditionally included the decision to consult with an appropriate professional (OB, other MDs, or another midwife) when a client’s situation or health status required additional information (“two heads are better than one”), or possible referral or transfer of care might be needed.
Not only are midwives aware that we don’t ‘practice medicine’, we also don’t want to practice medicine, which is why we trained in midwifery instead of going to med school. We want is to be a part of the mainstream healthcare system, with collegial connections to all kinds of doctors and nurse-midwives, other practitioners and medical services.
Conclusion:
 Ultimately, AB 1308 gave the obstetrical profession a statutory tool that recreated the social structure and power dynamics in which the physician is legally identified as “captain of the ship” who “gives the orders” and midwives (CNMs or LMs) are the “borrowed servants“.
Ultimately, AB 1308 gave the obstetrical profession a statutory tool that recreated the social structure and power dynamics in which the physician is legally identified as “captain of the ship” who “gives the orders” and midwives (CNMs or LMs) are the “borrowed servants“.
Personally, I think this whole system of underpaid, unappreciated “borrowed servants”/essential workers who serve at the pleasure of a system that disproportionately benefits and financially rewards medical doctors should be dismantled, including but not only the issues that concern mothers and midwives.
 Links to Pertinent Documents and other Reference
Links to Pertinent Documents and other Reference
EXCERPTS from the AMA‘S 2006 “Scope of Practice Partnership“ and links to their 2020 boast of “victory” in more than a dozen states, where they got the state legislatures to pass “physician extender” laws the legally define the role of nurse practitioners, nurse midwives, physical therapists, podiatrists, optometrists, psychologists, and several other non-physician practitioners as a class of indentured servants who are no longer professionals in their own right but are to function as “physician extenders” — that is, whose primary function is to serve the medical profession and only secondarily to serve their patients and the public:
RELEVANT AMA POLICY ~ Scope of Practice Partnership ~ HOD’s Resolutions
House of Delegate-160.949 – Practicing Medicine by Non-Physicians: states that “[o]ur AMA:
(1) urges all people, including physicians and patients, to consider the consequences of any health care plan that places any patient care at risk by substitution of a non-physician in the diagnosis, treatment, education, direction and medical procedures where clear-cut documentation of assured quality has not been carried out, and where such alters the traditional pattern of practice in which the physician directs and supervises the care given;
(4) continues to encourage state medical societies to oppose state legislation allowing non-physician groups to engage in the practice of medicine without physician (MD, DO) training or appropriate physician (MD, DO) supervision; and
(5) through legislative and regulatory efforts, vigorously support and advocate for the requirement of appropriate physician supervision of non-physician clinical staff in all areUas Uof medicine. (Res. 317, I-94; Modified by Res. 501, A-97; Appended: Res. 321, I-98; Reaffirmation A-99; Appended: Res. 240, Reaffirmed: Res. 708 and Reaffirmation A-00; Reaffirmed: CME Rep. 1, I-00).”
H-35.973 Scopes of Practice of Physician Extenders
Our AMA supports the formulation of clearer definitions of the scope of practice of physician extenders to include direct appropriate physician supervision and recommended guidelines for physician supervision to ensure quality patient care. (Res. 213, A-02)
H-35.988 Independent Practice of Medicine by “Nurse Practitioners”
The AMA, in the public interest, opposes enactment of legislation to authorize the independent practice of medicine by any individual who has not completed the state’s requirements for licensure to engage in the practice of medicine and surgery in all of its branches. (Sub. Res. 53, I-82; Reaffirmed: A-84; Reaffirmed: CLRPD Rep. A, I-92; Reaffirmed: BOT Rep. 28, A-03)
H-35.993 Opposition to Direct Medicare Payments for Physician Extenders
Our AMA reaffirms its opposition to any legislation or program which would provide for Medicare payments directly to physician extenders, or payment for physician extender services not provided under the supervision and direction of a physician. (CMS Rep. N, I-77; Reaffirmed: CLRPD Rep. C, A-89; Reaffirmed: Sunset Report, A-00)
Bibliography and References: set #2
Link to the end of an original essay entitled:
The Debate on Health Care Policy Reform ~ an exercise in pseudo-journalism
Links to PDF, beginning of Internet version, and other important topics:
PDF version to print or send to your Kindle of read on a smart phone with Kindle app
See Table of Contents & Links to each specific topics (separate page)
Five-Point Wrap Up:
The ABCs of a Political Action Plan
Excerpts from background materials:
Short-cut to: part 2, part 3, part 4, part 5, part 6, Wrap-up, references & background material
Tell-A-Vision for the 21st Cent
 Links to Dr. J. Whitridge Williams ~ Inventor of “elective hospitalization”, staring with middle- and upper-class white maternity patients whose families could afford to pay for a hospital birth, which included 14 days of “lying-in” care after the baby is born.
Links to Dr. J. Whitridge Williams ~ Inventor of “elective hospitalization”, staring with middle- and upper-class white maternity patients whose families could afford to pay for a hospital birth, which included 14 days of “lying-in” care after the baby is born.
Synopsis of Dr. J. Whitridge Williams’
‘Plan’ to finance a nationwide system of general hospitals using hospital-based maternity care as the “cash cow”
His well-meaning plan was to finance the replacement or incorporation of 8,000 two-to-ten bed privately owned hospitals run by one or two doctors as ‘for profit’ businesses, using the revenue generated by electively hospitalized healthy maternity patients, which cost very little to care for but can be charged the same daily fee as very sick patients that need a lot of attention from hospital employees and utilize a lot hospital supplies, equipment and services.
Dr. J. Whitridge Williams, author of “Williams Obstetrics” first published in 1904. After graduating from medical school in 1886, he trained as a gynecological surgeon, then spent 2 yrs in Europe in obstetrical and pathology clinical training programs. He was appointed Chief of Obstetrics at Johns Hopkins in 1899, and Dean of the Johns Hopkin’s School of Medicine in 1911. His book “Twilight Sleep: Simple Discoveries in Painless Childbirth” was published in 1914.
His big dream was to find a reliable way to finance a national system of general hospitals like the ones available for 200 years in Western Europe.
However, the AMA would never tolerate anything like the national systems paid for and often run by a national government. In an effort to generate a new and reliable revenue stream that could be used over the next decades to expand small privately-owned hospitals and build and equip new community general hospitals – one for every population center over 3,000 — and described by Dr. W “to as ubiquitous if not quite of numerous as libraries and school houses”).
To pay for this he came up with the idea of ‘elective hospitalization’.
He saw this as creating a large and steady stream of paying customers. The first demographic for elective hospitalizations were healthy middle- and upper-class maternity patients whose families well could afford to pay both the doctors’ fee a AND a hospital bill for a 14-day stay of mother in the maternity ward and the baby in the newborn nursery. Just one hospital labor and birth a day, with a 14-day stay for both mother and baby (total of 28 hospital days per birth) & equated to a maternity department pt. census of 9,800 days per year.
Inventing this income stream was an extraordinarily clever way generate money that would circumvent the politics of the AMA. Organized medicine in the US was opposed to anything that might interfere with its entrepreneurial view of medicine as a very lucrative & ‘no-holds-barred’ small business that could generate consider wealth from private physician fees. The AMA also rejected anything that smacked of “gov’t” meddling in the practice of medicine, which rejection of state or federal gov’t financing.
The AMA equated this to gov’t -run ‘socialized medicine’, which it hated. Without access to the non-gov’t sources of revenue from hospitalized healthy maternity patients, Dr. J. W. Williams knew the AMA would have killed his life-long dream — a nationwide system of well equipped , well-staffed general hospitals. From that standpoint, Dr. Williams scheme was masterful and he succeeded beyond his wildest dreams. What this meant for healthy childbearing women is a story for another day (see list of Tiny URLs at the bottom of this post that lead to the Dr. JWW’s personal and professional story)
Easy Shortcut to share –> https://tinyurl.com/y8pgewkg
You can link to each post or start with the “Intro” and link each of the following posts at the bottom to download next part.
Intro to 8-part series https://tinyurl.com/y8pgewkg
1 Intro to an 8-part series on Dr. Williams’ 1914 book “Twilight Sleep”: Simple Discoveries in Painless Childbirth”
2 Part 1: The Dream, the Motives, the Methods & Enduring Impact of 1914 book “Twilight Sleep ~ Simple Discoveries in Painless Childbirth ~ by famous American obstetrician: Part 1-a ~ Overview
3 The Dream, the Motives, the Methods & Enduring Impact of 1914 book “Twilight Sleep ~ Simple Discoveries in Painless Childbirth ~ by famous American obstetrician: Part 1 ~ Overview Easy-to-share Tiny URL >>> https://tinyurl.com/ycee9xv7
4 Dr. J.W. Williams: Part 2 ~ Inventing the Economic Engine for America’s private and corporate-owned Hospital System
Sorry, but you must click the link below for 2b instead of the post’s actual title: http://faithgibson.org/dr-j-w-williams-part-1-b-inventing-the-economic-engine-for-americas-private-and-corporate-owned-hospital-system/
5 Dr J. Whitridge Williams: Part 3 Elective Hospitalization ~ the basic economic unit for engine for America’s private system of hospitals
6 Dr. J. Whitridge Williams: Part 4 ~ Selling his odd ideas about childbirth to the public & philanthropists
7 There is a separate Tiny URL for Part 2-a ~ Dr. JWW’s Little Book and the Pentagon Papers <https://tinyurl.y8udohl6>
8 Dr. J. Whitridge Williams’ Little Book, the Pentagon Papers & movie “The Post”: Part 5 ~ Intro ~ profound harm caused by Twilight Sleep & Genera Anesthesia
9 Dr. J. Whitridge Williams’ Little Book & the Pentagon Papers: Part 6 Numbers don’t lie
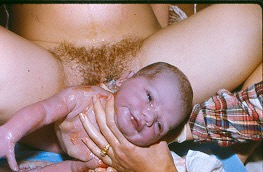
 The adoring eyes of the breastfeeding infant,
The adoring eyes of the breastfeeding infant,
as it gazes up into his/her mother’s eyes while lying peacefully in her arms, safe and secure. This is one of the best way to prepare a child so he or she can grow into intelligent and capable adult citizens, able to do his part in keeping our democratic country strong and
This is the true purpose and goal of the art and science of traditional, community-based, family-oriented midwifery!
AMA beware — Midwives, and dozens of other non-physician practitioners, will no longer quietly take our seat in the back of the bus, to be ‘seen and not heard‘ as a discriminated category of disenfranchised second class citizens.
We refuse to let your organization spend millions each year in illegitimate and illegal efforts to shore up an illegal monopoly by lobbying state legislature to pass newly restrictive licensing laws that define non-physician practitioners as “physician-extenders”, to function like a 19th century subservient wife or indentured servant.
Over the last 2 centuries, the allopathic medical profession in the US has developed for unexplained reasons, into a culture of harassment, a circumstance that historically begins in medical school when professors insult, belittle and upbraid medical students and those students quickly realize that uncivilized and insulting behavior