Dear Lilah *O*
I deleted the topics at very top, so this page looks different. Just start by clicking on the Yellowknife paper, which is now #1, then go on to read #2, #3, and #4. You can skip the “Early Unfinished Draft” link, which is only there so I can keep track of it and finish later.
warm regards, faith ^O^
Yellowknife Paper on the ethics of informed consent/decline in maternity care
This is an extraordinary paper on Informed Consent & Refusal for labor and births published in 2017 the journal BIRTH. It was written by a family practice physician actually attends births in a small community hospital in Yellowknife, BC, Canada.
Dr. Andrew Kotaska also posts on the Canadian “Maternity Care Discussion Group” (MCDG) moderated by Dr. Michael Klien, who’s been working hard to protect normal physiologic childbirth in healthy women for decades.
Since there are so many “Informed Consent” documents, and this one is so special, I have been referring to it as the “Yellowknife Paper“.
Yellowknife Pager –>Download PDF –> Informed-Consnt&Refusal_Kotaska BIRTH 2017

2. Final Version: Social & Political History of California Midwifery 1850 ~ 2014
3. Historical and contemporary comments by physicians about midwives ~ 1820 to Present
ADDENDUM: Photo and graphic history of Midwifery: 5,000 years ago to now
Early Unfinished Draft Part 2: The 400-year Disappearing Trick in which the mother-to-be is covered by sterile drapes, lying unconscious on her back, which the obstetrician performs a ‘baby-ectomy’; its mother is the only person in the delivery room that does not get to “attend” the birth of her baby

4. Part 3 Important Excerpts from legal precedents ~ Includes the following:
- ACOG Opinions no. 166 & 214 ~ Informed Consent & Maternal-fetal Relationship
- 2009 report on forced Cesarean
- Gabbe’s Obstetrics, ch 42 ~ Legal & Ethical Issues, Patient Rights
5. CCM Statement about VBAC ~ Subdirectory links ~ three-parts of Preamble & four-part VBAC Statement for California LMs
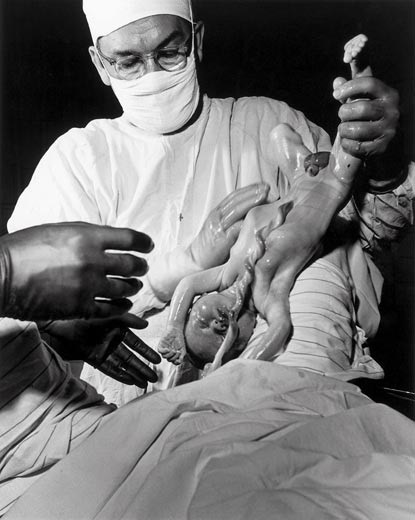
Below is the most amazing childbirth-related photo I’ve seen in decades. The picture below is a specially equipped and staffed operating room equipped to perform a cesarean hysterectomy for the life-threatening complication of placenta percreta.
This describes a potentially fatal form of abnormal placental implantation in which the placenta grows into the wall of the uterus and sometimes actually grows thru the uterus and implants on the mother’s bladder or other abdominal organs. The maternal mortality of this complication Btw 7 and 10% having a Cesarean hysterectomy
The high CS rate in the US has trigger such an increase in what formally was a very rare complication that there are now hospitals that specialize in performing this surgery. Note that 17 physicians, nurses and other essential hospital employees can be seen in this photo.
Did I mention the cost, over and above hospital care for a normal labor and birth? When I describe Cesarean surgery as the “gift that keeps on giving”, this is one of many examples.

@@@@@@@ archived copy of failed legislation @@@@@@@@@@@@
** PDF ~ DRAFT version SB 457** SB 457 (Bates) amends, 4-6-17
The formal version of the bill is to be printed on Monday, April 17th, and no doubt will quite different, so don’t get your undies in a bunch until you read the ‘real deal’.
1. Information ABOUT SB 457 by CAM-CALM board members (as of April 11th, 2017 @ 6 pm)
2. April 13th ~ PDF draft of SB457 {click here> SB 457 (Bates) amends, 4-6-17
This proposed language is the “mother of all bombs”, as it virtually destroys the practice of OOH midwifery, while also defining (i.e. limiting) the legal authority of LMs to OOH birth settings. If passed (it won’t be!) it would mean the two LMs with hospital privileges would no longer be able to authorized to practice mfry in a hospital setting.